Rotator Cuff Tears
Overview
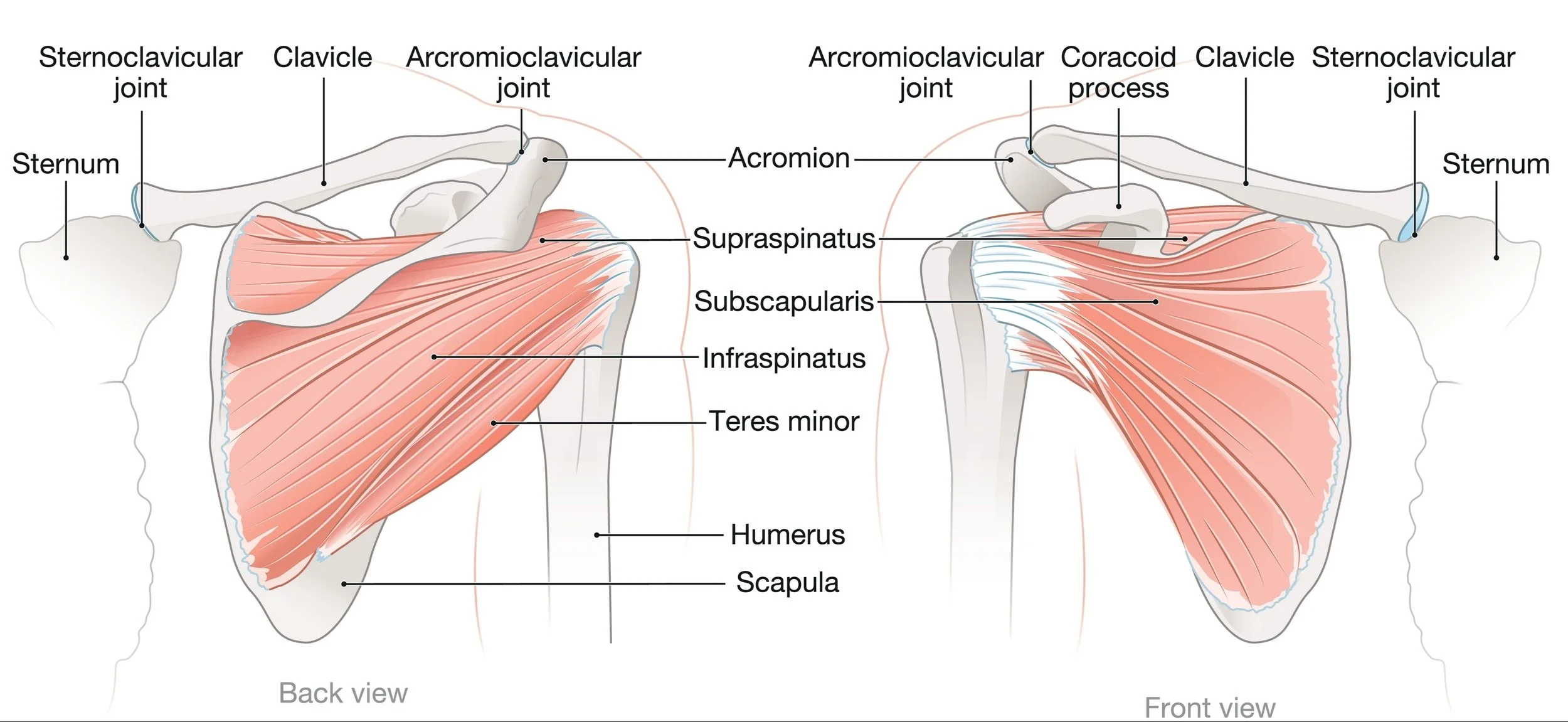
For patients in Richmond, VA seeking specialized care, understanding the mechanics of rotator cuff tears is the first step toward recovery. The rotator cuff is not a single muscle, but a complex of four distinct muscle-tendon units (supraspinatus, infraspinatus, subscapularis, and teres minor) that work together to surround the humeral head.
Think of the shoulder as a golf ball sitting on a golf tee. It is inherently unstable. The rotator cuff’s job is not just to lift the arm, but to compress the ball into the socket, creating a fulcrum and allowing for normal ball and socket mechanics. Without this compression, the large deltoid muscle would simply pull the arm bone upward into the roof of the shoulder, rather than lifting it away from the body. When a tendon tears, this "force couple" mechanism is disrupted, which can lead to pain and dysfunction. Since each of the four rotator cuff tendons attach at different points on the humerus, they all apply a different direction of force.
Rotator cuff tears are unique in that they can happen traumatically, such as in a fall, or they can happen slowly over time. Sometimes they are symptomatic and people have pain and difficulty moving their arm and sometimes they are asymptomatic and people don’t even know they’re there. Very frequently, other problems exist with rotator cuff tears such as a frozen shoulder, biceps tendonitis and shoulder arthritis. To diagnose a rotator cuff tear, we always begin with a physical exam but an MRI is often necessary to confirm the diagnosis.
For more information on this topic, see the American Academy of Orthopaedic Surgeon's educational page here.
Video courtesy of 3D Anatomy Lyon
Symptoms
Night Pain: This is the hallmark symptom of a rotator cuff tear. Patients often describe a deep ache that travels down the outside of the arm, making it challenging to sleep on the affected side.
Weakness: A specific inability to lift the arm away from the side or rotate it outward. In severe cases, the arm may drop when you try to hold it up and cannot be actively moved at all.
Pain with Motion: A "catch" or sharp pain when lifting the arm between 60 and 120 degrees.
Crepitus: A sensation of grinding or popping inside the joint, often indicating that the tear has allowed the bones to rub together.
The Spectrum of Tears: Understanding Your Injury
Treatment decisions are based entirely on the type of tear you have. Determining the type requires a discussion with a doctor and an MRI as sometimes what is perceived as an acute traumatic tear is actually an “acute-on-chronic” tear where the tendon was already chronically diseased and weakened and a trauma (such as a fall) finally completed the tear or made one that was already there symptomatic. An MRI helps evaluate for this and the treatment might change as a result of the findings. In general, rotator cuff tears fall into two categories: repairable and irreparable (not repairable).
1. Repairable Tears
A. Acute Traumatic Tears
The Scenario: You are an active person who fell on an outstretched arm or felt a "pop" while lifting. Immediately, you lost the ability to lift your arm.
The Subtypes: These are futher classified by which tendon(s) (supraspinatus, infraspinatus, subscapularis and teres minor) is/are torn and how far away from the bone the tendon now is (small, medium, large and massive). In this tear type, no matter how large the tear, it usually - but not always - is still repairable.
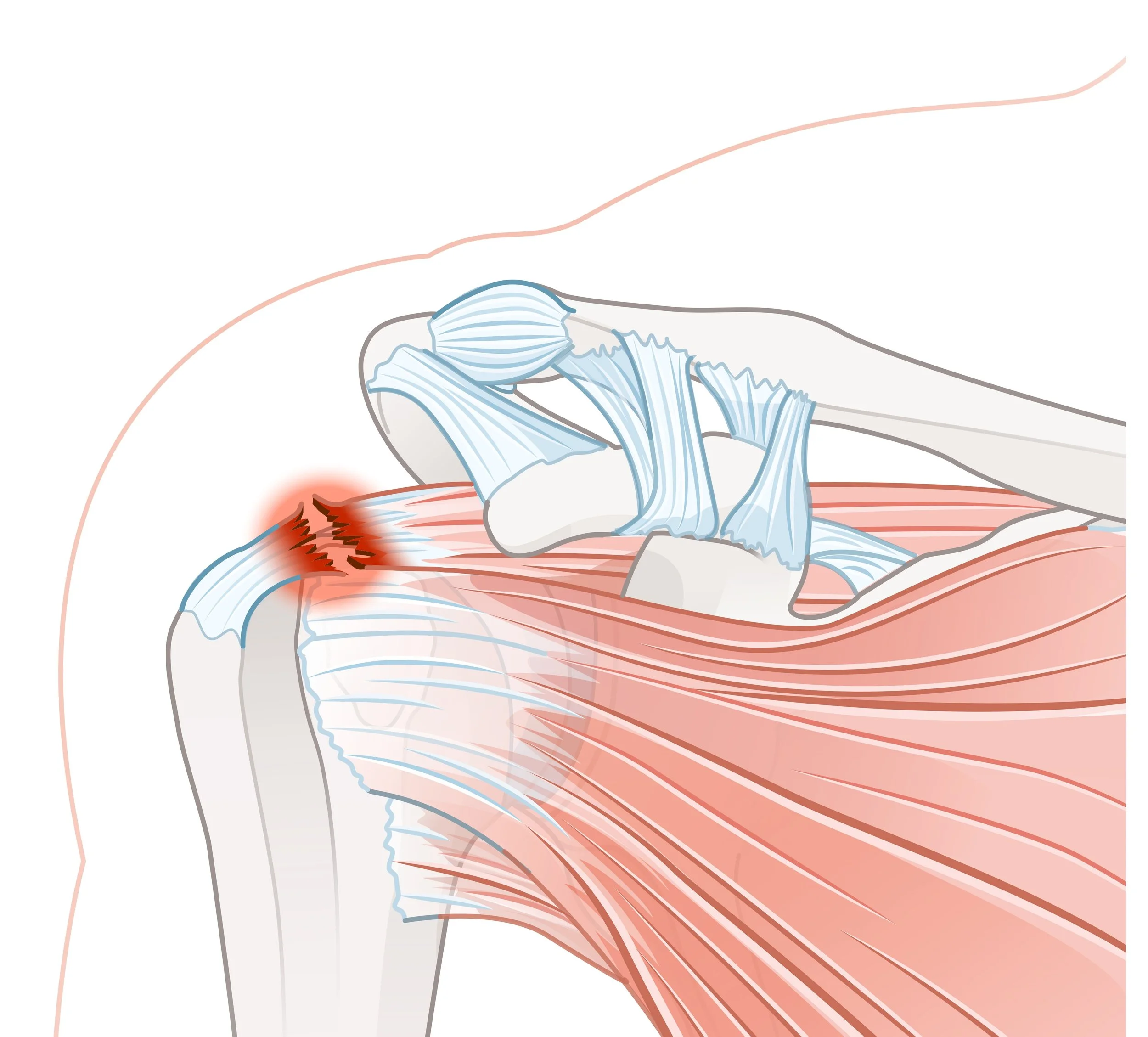
The Urgency: Unlike "wear-and-tear" fraying, acute traumatic tears are a surgical priority. The muscle is healthy, but the tendon has snapped off the bone.
Why We Don't Wait: "Time is Muscle." When a tendon snaps, the muscle belly immediately begins to retract (pull back). If left untreated, the muscle turns to fat (called fatty infiltration) and permanently loses its elasticity. Once this happens, the tear becomes irreparable.
Treatment: Semi-Urgent Arthroscopic Repair (ideally within 2-6 weeks) is recommended to restore anatomy. Like a broken bone, nonoperative treatment is usually skipped over in favor of surgery for these injuries, unless a patient is not able to, or not willing, to undergo the surgery for any reason.
B. Chronic Degenerative Tears (Wear and Tear)
The Scenario: You have had a dull ache for months that is slowly worsening. Motion might become progressively more difficult or altogether impossible.
The Biology: As we age, blood supply to the tendon diminishes. The tissue thins and frays like worn-out fabric and becomes more likely to tear, just as older clothes develop holes in them with time. Eventually the size of a tear might compromise the tendon’s ability to perform it's job compressing the humeral head into the socket and that is when motion becomes more difficult.
The Subtypes: These are futher classified by which tendon(s) (supraspinatus, infraspinatus, subscapularis and teres minor) is/are torn and how far away from the bone the tendon now is (small, medium, large and massive). In this tear type, the larger the tear, the harder it might be to repair it.
Treatment: These are initially managed with the non-operative protocols listed below. An arthroscopic rotator cuff repair is usually reserved for younger patients who fail therapy and have persistent pain and disability. In elderly patients, sometimes a reverse shoulder arthroplasty is a more appropriate option.
2. Irreparable Tears
Sometimes, a patient arrives too late. The tendon has retracted so far it cannot be stretched back to the bone reliably, and the muscle has turned to fat. In the past, these patients were told "nothing can be done." An MRI helps evaluate the repairabilty of a rotator cuff but sometimes only evaluation during surgery can provide an accurate assessment. There are two main types of irreparable rotator cuff tears: those with and without significant bony changes. When a rotator cuff tears, the ball-and-socket mechanics eventually stop working correctly and pseudoparalysis develops (the loss of motion). Sometimes this occurs immediately, sometimes after many years. If left long enough, the ball begins to contact the acromion (the roof of the shoulder) and the glenoid (socket) and these structures begin to erode. In this instance, a joint replacement becomes a more reliable solution.
A. No or Minimal Bony Changes
The Subtypes: These are futher classified by which tendon(s) (supraspinatus, infraspinatus, subscapularis and teres minor) is/are torn.
Treatment: These are initially managed with the non-operative protocols listed below. Surgery is usually reserved for patients who fail therapy and have persistent pain and disability.
Best For: Massive, irreparable tears of the top and back cuff muscles (supraspinatus/ infraspinatus).
The Procedure: Dr. Wall harvests the lower trapezius tendon from the back, extends it with an Achilles allograft, and attaches it to the humerus where the supra- and infraspinatus used to attac. This helps to rebalance the shoulder by restoring its force coupling, allowing it function with proper ball-and-socket mechanics again.
Best For: Massive tears of the front (Subscapularis).
The Procedure: Dr. Wall transfers this large back muscle’s tendon to the front of the humerus, where the subscapularis used to attach, to prevent the ball from sliding forward.
A Caveat: In some elderly patients, even when there are minimal bony changes, performing a tendon transfer may not be the best treatment solution and instead a reverse shoulder arthroplasty might be more appropriate.
B. Advanced Bony Changes
The Scenario: When a very large rotator cuff is left untreated long enough, the bones of the shoulder experience too much contact with each other and they begin to erode. This is often a painful process and motion is very limited during this time. It is called rotator cuff arthropathy. Once it’s at an advanced enough stage, the above tendon transfer options are no longer a good idea.
Treatment: These are initially managed with the non-operative protocols listed below. Surgery is usually reserved for patients who fail therapy and have persistent pain and disability.
The Solution: Reverse Shoulder Arthroplasty. By switching the ball and socket components, we change the physics of the shoulder, allowing the deltoid to power the arm without a rotator cuff.
Treatment Summary
Initial Non-Operative Treatment: Almost all rotator cuff tear treatment begins with non-operative management in the form of physical therapy, steroid injections, non-opiate pain medications and some degree of activity modification (if tolerated)
Rotator Cuff Repair – For acute, traumatic tears or symptomatic, chronic tears.
Lower Trapezius Tendon Transfer – For younger patients with massive, irreparable posterosuperior (supraspinatus and infraspinatus) rotator cuff tears with minimal bony changes
Latissimus Dorsi Tendon Transfer - For younger patients with massive, irreparable anterosuperior (subscapularis +/- supraspinatus) rotator cuff tears with minimal bony changes
Reverse Shoulder Arthroplasty – For elderly patients or for younger patients with more advanced bony changes