Biceps Tendonitis & SLAP Tears
Overview
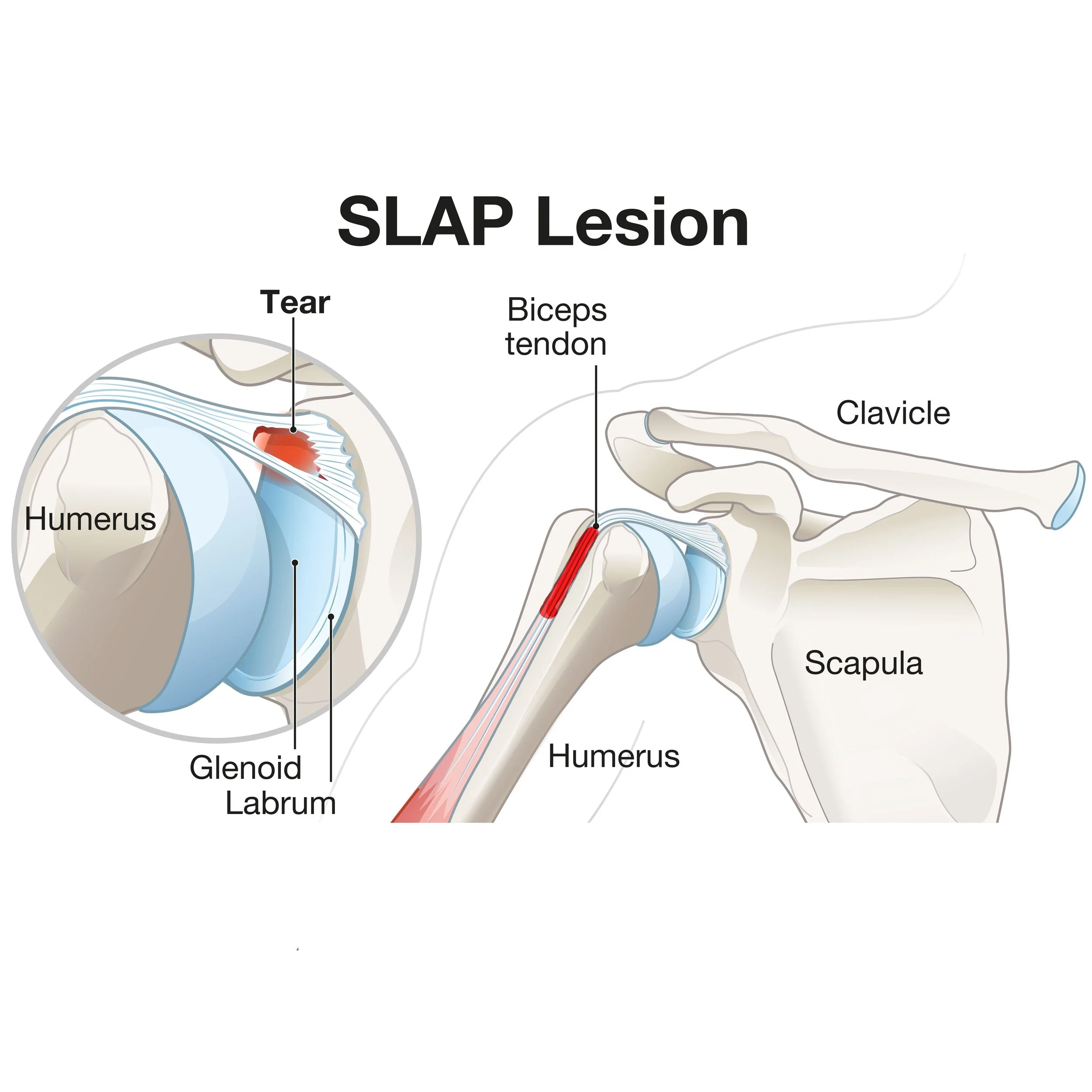
For patients in Richmond, VA seeking specialized care, understanding the mechanics of biceps tendonitis and SLAP tears is the first step toward recovery. When the Long Head of the Biceps (LHB) tears, it is a frequent source of anterior shoulder pain. This tendon travels up the front of the arm, through a small groove at the top of the humerus, takes a 90 degree turn and enters the shoulder joint, and attaches to the top of the socket at the labrum. Because of the sharp 90-degree turn as it enters the joint, it is prone to friction and fraying (see above image on the right with the highlighted red tendon inflammation at the top of the humerus)
A SLAP tear (Superior Labrum Anterior to Posterior) occurs where the biceps anchor (the superior labrum) pulls away from the bone (see above image on the left). While common on MRI scans in patients over 40 as just a product of aging, SLAP tears are also frequently found in overhead athletes due to the forces they put on these structures during sport. In older patients, the pain is usually from the biceps tendon itself (tendonitis) rather than the labral tear but both of these problems can, and often do, occur simultaneously and can usually be treated the same.
It is also important to note the close relationship between the long head of the biceps and the subscapularis tendon, which is one of the four rotator cuff muscles. Both of these structures live right on the front of the shoulder - the subscapularis attaches to a small part of the humerus called the lesser tuberosity, which also forms one of the walls of the bicipital grove. Oftentimes, if there is a problem with one of these structures - the biceps tendon and the subscapularis - there can be a problem with the other one, such as a tear in the subscapularis. Sometimes this can be determined by your doctor during your exam but it often requires an MRI to make the diagnosis.
For more information on biceps tendonitis, see the American Academy of Orthopaedic Surgeon's educational page here.
For more information on SLAP tears, see the American Academy of Orthopaedic Surgeon's educational page here.
Symptoms
Groove Pain: Pain at the front of the shoulder (the bicipital groove) that travels down the biceps muscle.
Pain with Shoulder Motion: Some patients also feel pain in their shoulder when the reach backwards or behind their back.
Clicking: A deep click or pop when rotating the arm can sometimes be felt if the tendon is able to snap in and out of its grove.
Popeye Deformity: If the tendon ruptures completely, the muscle bunches up in the arm (often painless after the initial snap).
Non-Operative Management
Medication: If safe for the patient, anti-inflammatories (NSAIDs) are part of the first-line treatment for this problem that is usually inflammation-driven.
Ultrasound-Guided Injection: Steroid injections are anti-inflammatory, just like NSAIDs. By using ultrasound to ensure the steroid injection enters the very small bicipital grove, we can be sure that we accurately target the biceps tendon exactly at the site where it is often inflammed.
Tenotomy (Autotenodesis): In some older patients, if the tendon ruptures spontaneously, the pain usually disappears. Most patients are satisfied with this outcome but it can result in the Popeye deformity mentioned above and have some mild cramping for a few months. Some patients want this addressed surgically for cosmetic reasons.
When is Surgery Needed?
Persistent Anterior Shoulder Pain: When pain limits daily life or recreational activities despite medications, activity modification and steroid injections.
Persistent Pain and Deformity after Spontaneous Tenotomy: If the tendon spontaneously ruptures and a patient is highly dissatisfied with the cosmetic appearance of their arm and have ongoing pain then surgery may be considered but it is dependent on the age since the spontaneous rupture. Attempting surgery long after the rupture when the tendon will have scarred into place can be invasive, dangerous and not reliably produce the desired outcome.
SLAP Tears in Athletes: Throwing athletes who lose velocity or control.
Surgical Solutions
Biceps Tenodesis – An arthroscopic surgery where Dr. Wall moves the tendon attachment out of the joint to solid bone. The segment of inflammed tendon between the old and new attachment sites is no longer needed and so it is removed. This eliminates any pain from the SLAP tear and the inflammed tendon.
SLAP Repair – An arthroscopic surgery where Dr. Wall re-anchors the superior labrum to the glenoid (the socket of the shoulder joint). This is reserved mostly for young athletes.