Coracoplasty
The Goal
Dr. Kevin Wall provides specialized, fellowship-trained surgical treatment for Arthroscopic Coracoplasty to restore function and relieve pain for patients in Richmond, VA, and the surrounding Central Virginia communities. The goal of this procedure is to decompress the subcoracoid space, where the coracoid process can abnormally "impinge" upon the subscapularis tendon or the long head of the biceps. While traditionally performed for subcoracoid impingement, this is also a useful tool in patients with a Reverse Shoulder Arthroplasty (RSA) who experience persistent pain at the front of their shoulder. In the setting of RSA, the altered mechanics can cause the humeral component or the remaining soft tissues to contact the coracoid and/or the conjoined tendon. By precisely contouring the bone and, when necessary, performing a conjoined tendon relocation, we can eliminate this mechanical conflict while maintaining the essential tension of the surrounding musculature.
This page is designed to educate you specifically about this procedure. Additional information that generally applies to most of Dr. Wall’s surgeries can be found on these pages:
The Procedure
The Approach: Performed arthroscopically (minimally invasive) using standard shoulder portals.
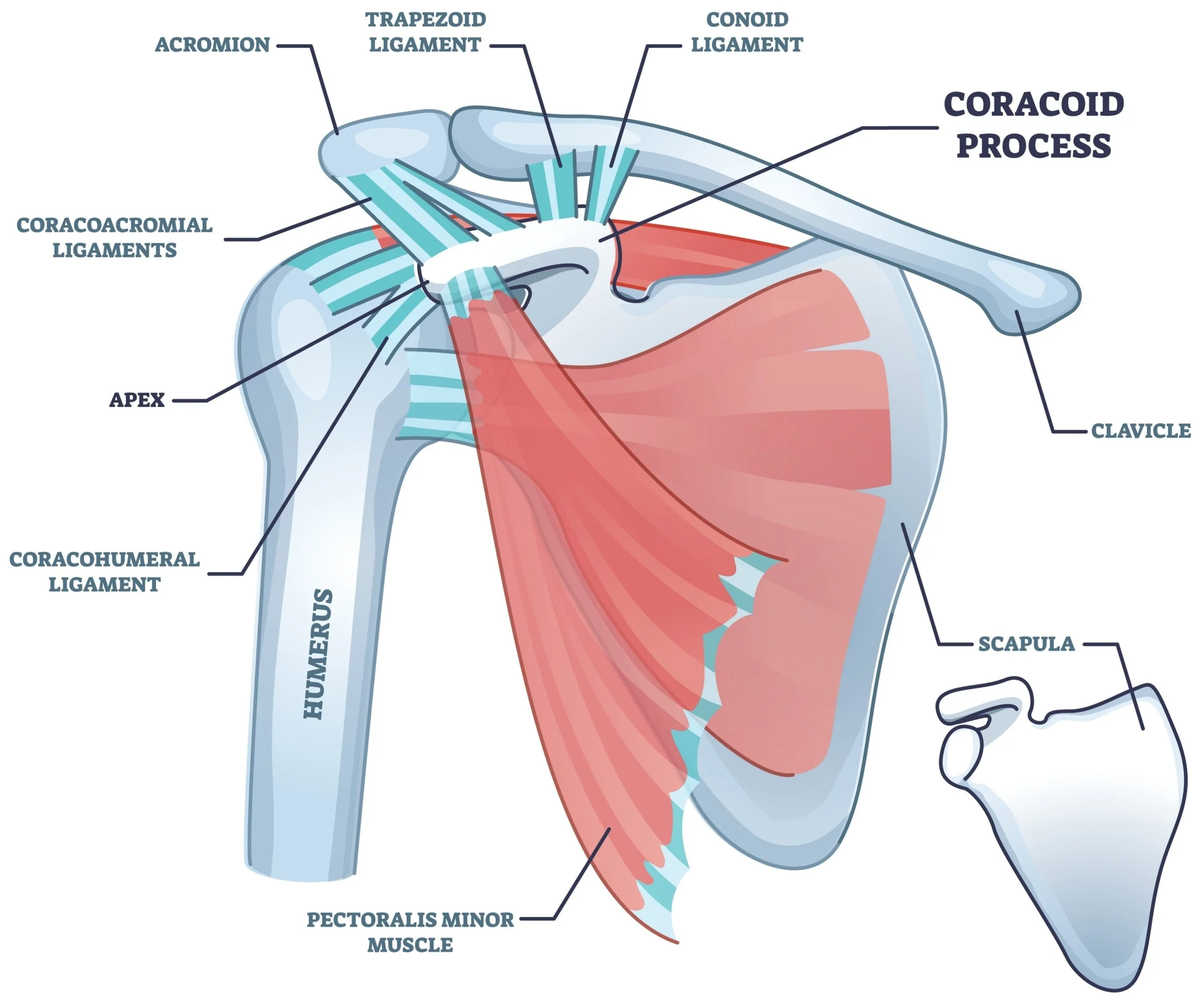
Coracoplasty: Using a specialized high-speed surgical burr, Dr. Wall removes part of the coracoid process (usually just the apex labeled in the above image). This removes the part of this bone that was causing the impingement with the subscapularis or the reverse shoulder arthroplasty.
Conjoined Tendon Relocation: In cases of persistent anterior impingement—especially in RSA—the conjoined tendon (short head of the biceps and coracobrachialis) may be relocated. This is because the RSA’s humeral component usually contacts the apex of the coracoid, where the conjoined tendon attaches (not shown in the above illustration). In order for the apex to be removed, something must be done to the conjoined tendon. The relocation involves carefully detaching the tendon from the coracoid and re-anchoring it in a tension-neutral position to preserve muscle length.
Subscapularis Evaluation: The underlying subscapularis tendon is inspected for any secondary tearing or fraying caused by the chronic impingement and repaired if necessary.
Post-Op Protocol
Immobilization (Phase 1: 0–2 weeks): A sling is utilized for comfort. Gentle motion of the shoulder begins, progressing from passive to active-assisted, and eventually active motion as tolerated. Elbow, wrist, and hand motion are encouraged as tolerated. No lifting, pushing, pulling, or weightbearing is permitted during this initial phase.
Formal Physical Therapy: Professional therapy sessions are initiated at post-operative Week 1.
Phase 2 (2–8 weeks): Ongoing shoulder motion continues as tolerated. Progressive stretching and strengthening begin using resistance bands at the shoulder. If a conjoined tendon relocation was performed, resisted elbow flexion and forceful extension are strictly limited to protect the repair.
Phase 3 (8 weeks+): Stretching and strengthening exercises continue, progressing to weights as tolerated, including exercises for the elbow.
When to Seek Care
You should schedule a consultation if:
You have persistent pain in the front of your shoulder that worsens when you reach across your body or rotate your arm inward.
You have had a Reverse Shoulder Arthroplasty (RSA) but continue to experience a sharp, anterior "catching" or pain that hasn't responded to therapy.
You feel a painful "clunk" or "snap" in the front of your shoulder during certain movements.