RHOMBOID REPAIR
The Goal
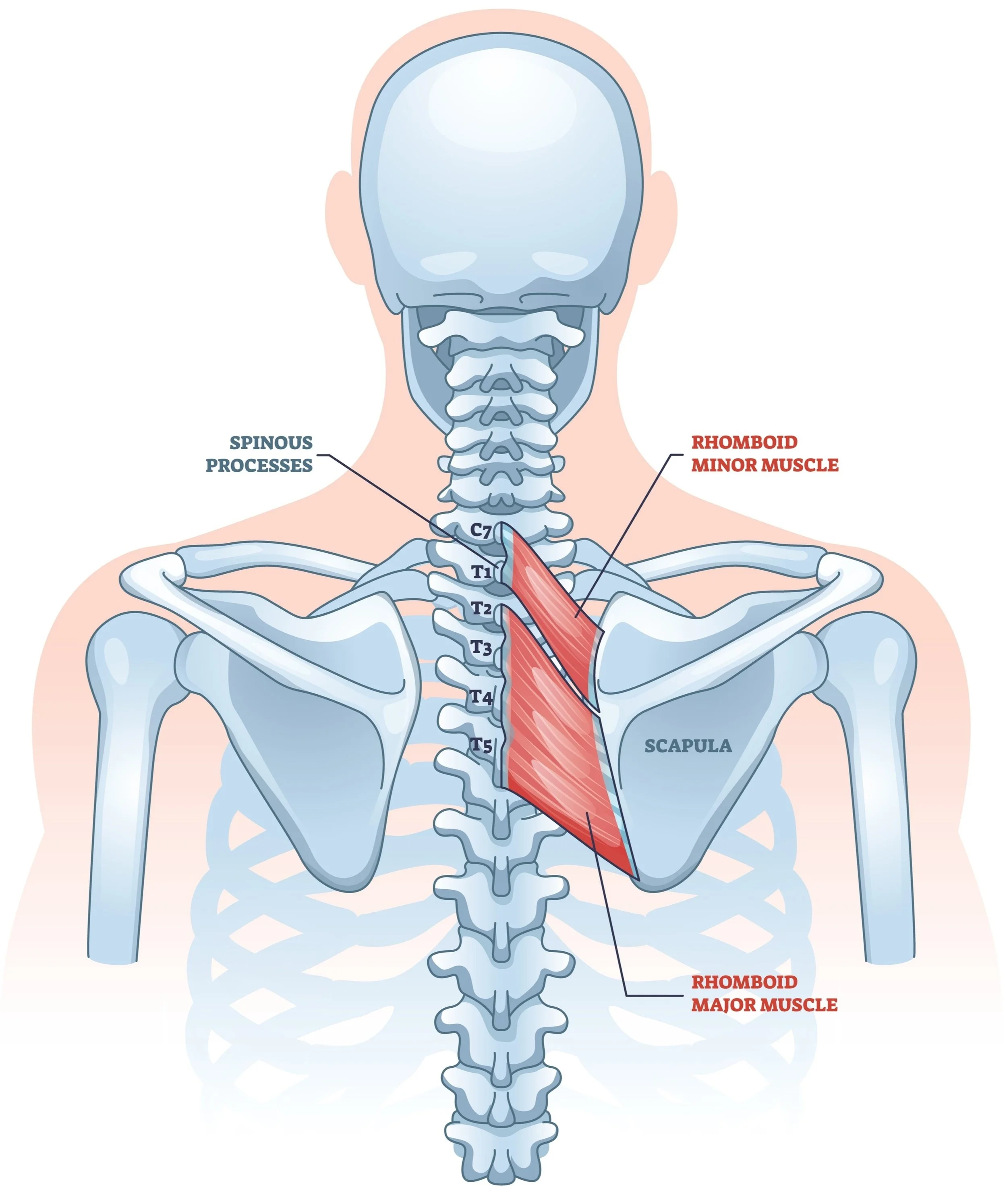
Dr. Kevin Wall provides specialized surgical treatment for Rhomboid Tendon Tears to relieve chronic, focal pain and restore scapular stability for patients in Richmond, VA, and the surrounding Central Virginia communities. The rhomboid muscles are essential for pulling the shoulder blade back toward the spine. When these muscles tear away from the bone—either from a traumatic injury or as a complication of a previous surgery—it causes a distinct, focal pain at the inner edge of the shoulder blade that makes sitting or driving difficult. The goal of this procedure is to physically reattach the torn muscle to the scapula, eliminating the painful gap and restoring the tension required for normal shoulder movement.
This page is designed to educate you specifically about this procedure. Additional information that generally applies to most of Dr. Wall’s surgeries can be found on these pages:
The Procedure
This surgery is reserved for patients with a confirmed structural defect (tear) who have failed conservative management. It is particularly indicated for:
Traumatic Avulsions: Acute detachments caused by high-energy injuries (e.g., wrestling, weightlifting).
Post-Surgical Dehiscence: Repairing the muscle attachment if it was damaged or detached during a prior scapulothoracic endoscopy (a known complication where the "scope" portals injure the rhomboid insertion).
The Technique
Open Approach: Unlike many shoulder surgeries that are arthroscopic, a rhomboid repair requires an open incision. Dr. Wall makes a vertical incision along the medial (inner) border of the scapula to directly visualize the damaged muscle.
Mobilization: The retracted edge of the rhomboid muscle is identified and freed from any scar tissue.
Bone Preparation: The edge of the scapula is prepared to create a "bleeding bone" surface, which is critical for biological healing.
Anchor Fixation: Dr. Wall inserts high-strength suture buttons into the bone of the scapula. The sutures are passed through the torn muscle tendon and tied down, firmly compressing the muscle back against the bone to allow it to heal in its anatomic position.
Post-Op Protocol
Because this is a tendon-to-bone repair (similar to a rotator cuff repair), biological healing takes time. You must protect the repair while it heals.
Immobilization (Phase 1: 0–6 weeks):
Sling: You must wear a sling at all times, including while sleeping, to keep the shoulder blade supported and prevent the muscle from pulling away.
Restrictions: Absolutely no reaching behind the back and no rowing motions (pulling the shoulder blades together).
Hygiene: You may remove the sling carefully for showering, keeping the arm close to the body.
Formal PT Start: Professional physical therapy typically begins at Post-Op Week 6.
Phase 2 (6–12 weeks):
Motion: The sling is discontinued. Therapy focuses on gentle passive and active-assisted range of motion.
Scapular Control: Exercises to retrain the scapula without putting heavy load on the rhomboids.
Phase 3 (12+ weeks):
Strengthening: Progressive strengthening begins.
Return to Sport: Full return to heavy lifting or contact sports is typically cleared around 4–6 months, once the tendon is fully matured.
When to Seek Care
You should schedule a consultation if:
You have persistent, pinpoint burning pain between your spine and shoulder blade that you can cover with one finger.
You feel a painful "step-off" or gap along the edge of your shoulder blade.
You developed new, sharp back pain immediately after a scapulothoracic surgery.
You have been told your MRI is normal, but you still have severe focal pain when pulling your shoulders back.