RHOMBOID MUSCLE INJURY
Overview
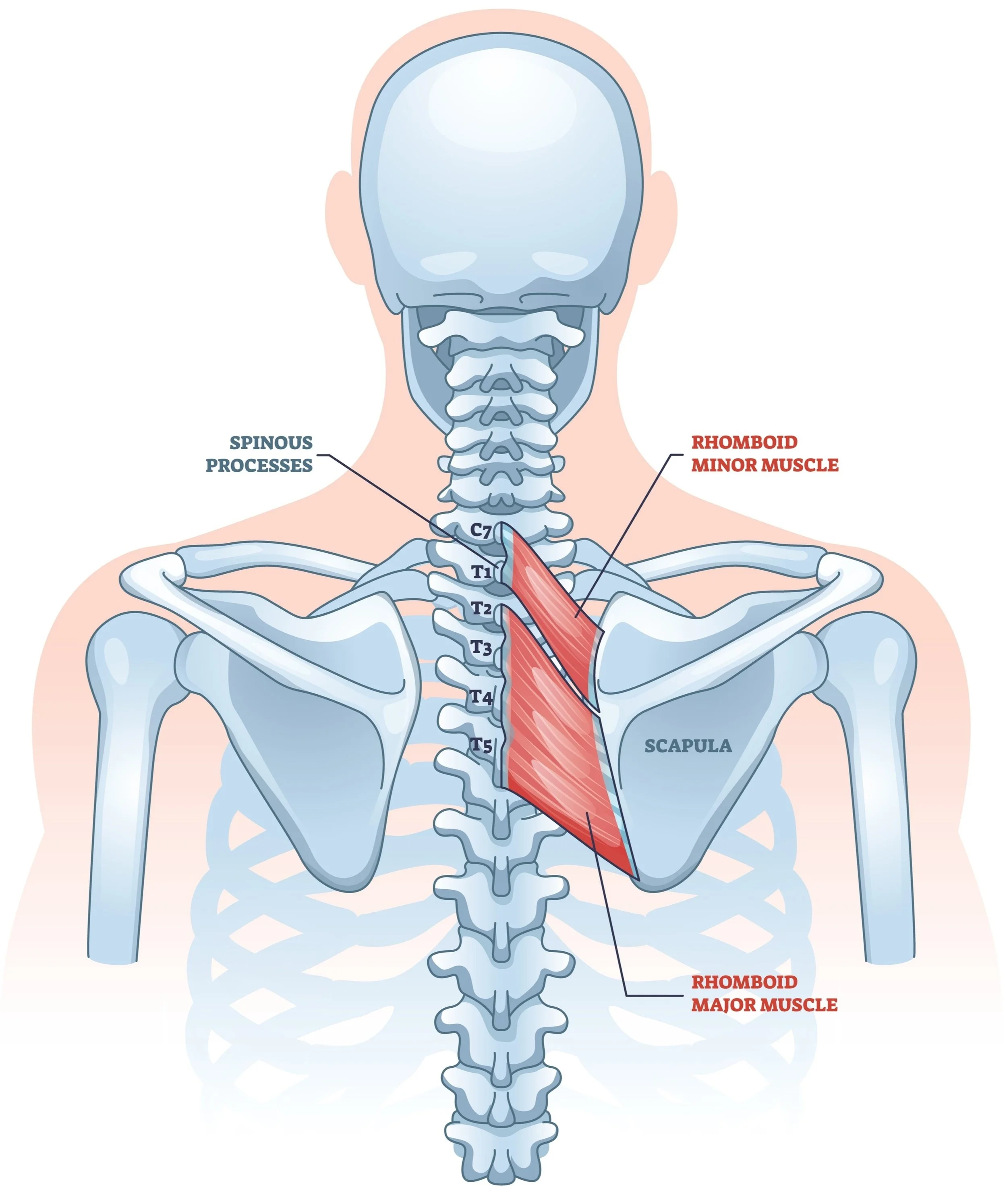
Dr. Kevin Wall provides specialized evaluation and treatment for rhomboid injuries to relieve focal pain and restore scapular stability for patients in Richmond, VA, and the surrounding Central Virginia communities. The rhomboid muscles (major and minor) are the primary retractors of the scaupla (the shoulderblade), pulling it toward the spine. Injuries to these muscles are frequently overlooked or misdiagnosed as "muscle spasms" or "knots." While often small in size, a tear or chronic strain in the rhomboid can cause debilitating, pinpoint pain that makes sitting, driving, or working at a computer unbearable.
The Problem
Rhomboid injuries typically fall into one of two categories, both resulting in a disruption of the muscle fibers at their attachment on the medial (inner) border of the scapula.
1. Traumatic & Atraumatic Tears
Traumatic: A sudden injury, such as a high-velocity throw, a fall, or a heavy lift, can cause an acute tear where the muscle pulls away from the bone.
Atraumatic (Repetitive): Chronic poor posture or repetitive rowing motions can cause micro-tearing and focal inflammation at the insertion point.
2. Iatrogenic (Post-Surgical) Injury
A specific and often unrecognized cause of rhomboid pain is prior scapulothoracic arthroscopy. If the surgical portals (incisions) were placed too medially during a previous "scapula scope," or if the resection of a bursa was too aggressive, the rhomboid attachment can be damaged or partially detached. Patients often report that their original snapping sensation is gone, but they now have a new, burning pain closer to the spine.
The Diagnostic Challenge
Rhomboid injuries are notoriously difficult to diagnose for two reasons:
The MRI "Blind Spot": The rhomboid muscles are very thin and located on the far edge of a standard shoulder MRI field of view. Because standard MRI slices are relatively thick, a small tear or focal inflammation can easily be "skipped over" or look completely normal on the scan.
Mimics: The symptoms often mimic nerve entrapment (dorsal scapular nerve) or back issues.
Symptoms & Examination
Focal, Pinpoint Pain: Unlike the generalized ache of a neck strain or the long straight course of a dorsal scapular nerve entrapment, patients can usually point to the exact spot of pain along the vertical inner edge of the shoulder blade.
Pain with Retraction: Pulling the shoulders back (rowing motion) sometimes reproduces the sharp pain.
Palpable Defect: In severe tears, a small gap or "step-off" can be felt along the edge of the scapula.
Treatment Options
Non-Operative Management
The vast majority of rhomboid injuries heal with dedicated conservative care.
Ultrasound-Guided Injections: Placing a steroid injection directly into the focal area of pain can reduce inflammation and pain.
Specialized Physical Therapy: Focusing on scapular positioning and off-loading the injured muscle.
Surgical Repair
Surgery is rare but effective for refractory cases, particularly acute traumatic detachments or painful post-surgical dehiscence.
Open Rhomboid Repair: Dr. Wall performs an open procedure to identify the torn or scarred muscle edge and re-anchor it to the scapula using heavy-duty sutures and bone anchors. This restores the tension and stability of the muscle.
When to Seek Care
You should schedule a consultation if:
You have sharp, pinpoint pain between your spine and shoulder blade that hasn't gone away with massage or rest.
You developed new pain near your spine after undergoing a scapulothoracic endoscopy (scope) procedure.
You have had an MRI of your shoulder that was read as "normal," but you still have severe focal pain.