AC Joint Injury(Shoulder Separation)
Overview
For patients in Richmond, VA seeking specialized care, understanding the mechanics of AC joint injuries is the first step toward recovery. An acromioclavicular (AC) joint injury (also called a shoulder separation) is a traumatic injury where the ligaments holding the collarbone (clavicle) to the shoulder blade (scapula) are torn. Unlike a "dislocated shoulder" (where the ball pops out of the socket), a separation involves the clavicle springing upwards because its tether (the coracoclavicular ligaments) has snapped. These ligaments connect the undersurface of the clavicle to a small bony prominence on the scapula called the coracoid (hence, coracoclavicular ligaments).
This injury is most commonly seen in contact sports (football, hockey, lacrosse) or cycling and skiiing accidents where the patient lands directly on the "point" of the shoulder. The force drives the shoulder blade down, but the collarbone stays up, creating a stepped deformity. While this deformity is sometimes visible, the diagnosis must be made with x-rays.
For more information on this topic, see the American Academy of Orthopaedic Surgeon's educational page here.
Symptoms
Pain: Sharp pain on top of the shoulder, especially when trying to lift the arm or reach across the chest.
The Bump: A distinct, hard lump on top of the shoulder. In severe cases, the skin may feel tight or "tented" over the bone.
Instability: A feeling that the arm is heavy or dragging.
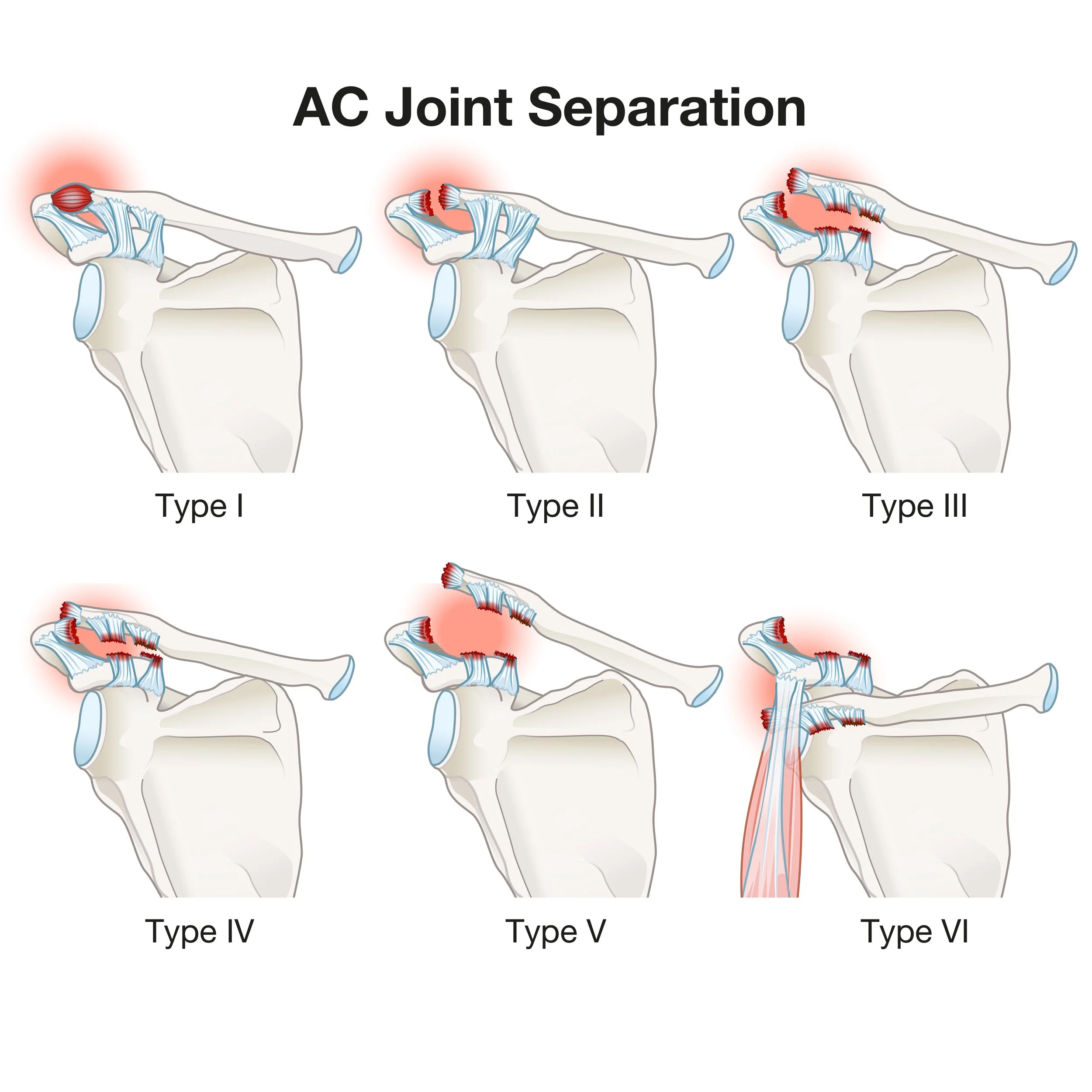
The Classification (Rockwood Scale)
Type I & II: Sprains or partial tears. The bump is small or nonexistent.
Type III: Complete tear of all ligaments. The collarbone is elevated (displaced) up to 100%.
Type IV, V, VI: Severe displacement where the clavicle is further displaced (more than 100%) or punctures muscle or skin.
Non-Operative Management
Benign Neglect: The vast majority of Type I, II, and even some Type III injuries can be treated without surgery. The "bump" may remain permanent, but the pain typically subsides once the inflammation settles (6-12 weeks).
Sling & Rehab: Short-term immobilization followed by scapular strengthening.
When is Surgery Needed?
High-Grade Injuries (Type IV-VI): These almost always require surgery because the bone is trapped or threatening the skin or chronic disability is anticipated.
Painful Type III: In overhead athletes or manual laborers, the lack of connection between the acromion and clavicle can cause chronic fatigue and pain. In patients with lower demands, a trial of nonoperative management is usually recommended first.
Chronic Instability/Pain: If the shoulder feels unsupported years after the injury or remains persistently painful.
Surgical Solutions
The exact surgery offered depends on how old the injury is but the goal is the same: to restore the connection between the scapula and the clavicle at the location where the coracoclavicular ligaments are.
Coracoclavicular Ligament Reconstruction, which may utilize a reinforcing tendon graft for more chronic injuries